The debt talks in Washington are slowly dying as the deficit continues to drop at one of the fastest rates in history. Thankfully then, we can begin to fight those attempting to hurt the poor and make cuts on working families. But we have to remain serious on one point. Entitlement spending, most notably on health services, has become unsustainable as we debate our plan for caring for America’s vulnerable. This debate, as partisan as it has become, undoubtedly converges on a central point: health care inflation must be slowed. One prominent tactic is increasing physician to patient transparency in price and efficacy. Yet, acknowledging the weaknesses of this “knowledge is power” approach will be necessary as we consider an improved American opportunity for all.
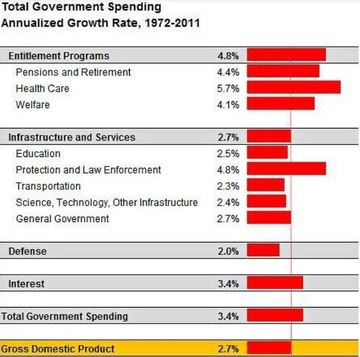
Entitlement growth is not a new challenge for the United States. When Nate Silver of the NYTimes indulged on “What is Driving Growth in Government Spending,” he portrayed the path we have been on since 1972 with health care far outpacing our gross domestic product (shown in graphic). The 5.7% displayed is mainly the growth rate of Medicare and Medicaid, including inflation rates as well as program expansions. Not only is this a problem for the deficit itself, it is a problem for other competing programs (like education and science/technology) which are subsequently controlled to make room for our growing health care responsibilities. This, in turn, hurts American opportunity by reducing the resources we have to remain competitive and train the next generation of American workers.
Now, health care inflation as of late has begun to decline. Drivers are still being analyzed for their contribution, including Medicare provisions included in the Affordable Care Act and the effects of the Great Recession, but while the ACA provisions and the expansion of Medicaid (instead of more costly plan subsidies) are helping the government payout, there has been no comprehensive plan for private-market inflation. This is the focus for the future, since the CBO analysis shows health care spending as a percentage of GDP growing from 4.6% today to 5.9% in 2023.
This is a topic where we should turn to the health actuary community. When the SOA surveyed over 3000 members of the SOA health section living in the United States, transparency was a clear favorite for cost control. There were three parts of this transparency: price visibility, efficacy of care education for patients, and visible measures for efficacy of care. The goal is to allow patients to perform cost/benefit analysis for their procedures and prescriptions, to form a way to publicly measure the performance of physicians and hospitals, and consciously limit the amount of unnecessary or unnecessarily expensive care. The most important piece will be the education of patients on efficacy of treatment. There has been mounting evidence that public information may be ignored or not trusted if patients are not educated on its benefits and uses.
This type of public information has been slowly making its way to the federal level, and some states have been ready to implement. The Report Card on State Price Transparency Laws has only awarded top marks to two states: Massachusetts and New Hampshire. The A-rating was given for the implementation of shared information on a public website of inpatient/outpatient services for both doctors and hospitals, as well allowing patients to request information before hospital admission. The state-reported effect has been lower costs, improvement of quality, and the empowerment of the patient. All this leads to the conclusion that price and efficacy transparencies are a no-brainer, but let’s think about some of its consequences.
Since the thought of price and quality transparency is not a new one, the academic world has had time to research its possible negative consequences. One of these studies looked specifically at the effect of transparency on cardiac surgeons. The conclusion was troubling. Surgeons, in order to secure solid efficacy scores, were acting more exclusionary to patients in poorer health than they had been before the scores. Not only harder on the sick, but perceptions of certain races and low-income citizens’ ability to fulfill patient roles in treatment led to more exclusionary practices. Now, is it possible that new stringent rules and cost restraints with Medicare and Medicaid could be contributing to the perceived exclusion of minority races and low-income individuals? Possibly, but the discriminatory perception has been shown (substantially) even in single-payer systems where the financial consequence has no effect on doctor choices. These possible discriminatory outcomes are ones that have to be a key part of the transparency discussion if we want to reduce our federal deficit in an ethical way.
Susan Pantely, FSA, MAAA , alongside the 2010 SOA actuarial survey, said that our challenges in the health care system have to be met with a strategy that “…reduces costs while improving quality.” Our high and rising national debt is a problem that is universally unwanted, but politically entangled. Regardless of the future restructuring of our entitlement programs, health care inflation is a certain focal point. The empowerment of patients on their price and physician choices is a big step, but without patient protection from discrimination, we may be accepting an economic gain at the cost of further segregating and hurting an already-vulnerable group of Americans. So, to extend Pantely’s quote, the future of solving America’s health care inflation problem requires the reduction of cost and improvement of quality for all.
Entitlement growth is not a new challenge for the United States. When Nate Silver of the NYTimes indulged on “What is Driving Growth in Government Spending,” he portrayed the path we have been on since 1972 with health care far outpacing our gross domestic product (shown in graphic). The 5.7% displayed is mainly the growth rate of Medicare and Medicaid, including inflation rates as well as program expansions. Not only is this a problem for the deficit itself, it is a problem for other competing programs (like education and science/technology) which are subsequently controlled to make room for our growing health care responsibilities. This, in turn, hurts American opportunity by reducing the resources we have to remain competitive and train the next generation of American workers.
Now, health care inflation as of late has begun to decline. Drivers are still being analyzed for their contribution, including Medicare provisions included in the Affordable Care Act and the effects of the Great Recession, but while the ACA provisions and the expansion of Medicaid (instead of more costly plan subsidies) are helping the government payout, there has been no comprehensive plan for private-market inflation. This is the focus for the future, since the CBO analysis shows health care spending as a percentage of GDP growing from 4.6% today to 5.9% in 2023.
This is a topic where we should turn to the health actuary community. When the SOA surveyed over 3000 members of the SOA health section living in the United States, transparency was a clear favorite for cost control. There were three parts of this transparency: price visibility, efficacy of care education for patients, and visible measures for efficacy of care. The goal is to allow patients to perform cost/benefit analysis for their procedures and prescriptions, to form a way to publicly measure the performance of physicians and hospitals, and consciously limit the amount of unnecessary or unnecessarily expensive care. The most important piece will be the education of patients on efficacy of treatment. There has been mounting evidence that public information may be ignored or not trusted if patients are not educated on its benefits and uses.
This type of public information has been slowly making its way to the federal level, and some states have been ready to implement. The Report Card on State Price Transparency Laws has only awarded top marks to two states: Massachusetts and New Hampshire. The A-rating was given for the implementation of shared information on a public website of inpatient/outpatient services for both doctors and hospitals, as well allowing patients to request information before hospital admission. The state-reported effect has been lower costs, improvement of quality, and the empowerment of the patient. All this leads to the conclusion that price and efficacy transparencies are a no-brainer, but let’s think about some of its consequences.
Since the thought of price and quality transparency is not a new one, the academic world has had time to research its possible negative consequences. One of these studies looked specifically at the effect of transparency on cardiac surgeons. The conclusion was troubling. Surgeons, in order to secure solid efficacy scores, were acting more exclusionary to patients in poorer health than they had been before the scores. Not only harder on the sick, but perceptions of certain races and low-income citizens’ ability to fulfill patient roles in treatment led to more exclusionary practices. Now, is it possible that new stringent rules and cost restraints with Medicare and Medicaid could be contributing to the perceived exclusion of minority races and low-income individuals? Possibly, but the discriminatory perception has been shown (substantially) even in single-payer systems where the financial consequence has no effect on doctor choices. These possible discriminatory outcomes are ones that have to be a key part of the transparency discussion if we want to reduce our federal deficit in an ethical way.
Susan Pantely, FSA, MAAA , alongside the 2010 SOA actuarial survey, said that our challenges in the health care system have to be met with a strategy that “…reduces costs while improving quality.” Our high and rising national debt is a problem that is universally unwanted, but politically entangled. Regardless of the future restructuring of our entitlement programs, health care inflation is a certain focal point. The empowerment of patients on their price and physician choices is a big step, but without patient protection from discrimination, we may be accepting an economic gain at the cost of further segregating and hurting an already-vulnerable group of Americans. So, to extend Pantely’s quote, the future of solving America’s health care inflation problem requires the reduction of cost and improvement of quality for all.
 RSS Feed
RSS Feed
